 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
LUNGS, BRONCHI AND TRACHEA
The lungs (Lat. pulmo), which are enclosed in the pleura, fill up nearly the whole chest cavity. The lungs are connected together by the windpipe (trachea) and the two main bronchi. The right lung is made up of three pulmonary lobes (lobi), and the left lung is made up of two. The smallest units of the lungs are the 300-400 million microscopic endodermal air sacs called alveoli, which together constitute a breathing surface of 80-100m². The alveoli are where the actual taking in of oxygen and giving off of carbon dioxide take place.
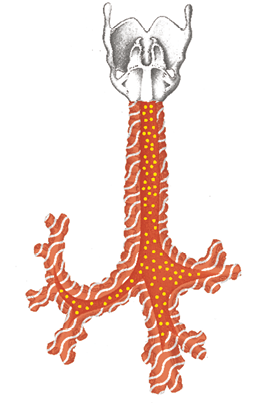
The wind pipes and bronchial tubes are made of cartilage and are lined with ectodermal epithelium. They belong to territorial areas controlled by the cerebral cortex.
The endodermal mucus producing goblet cells sit everywhere in the windpipe and bronchial tubes and provide the breathing apparatus with moisture.
Bronchial Mucosa
Territorial-fear conflict
Alveoli
Fear-of-death conflict
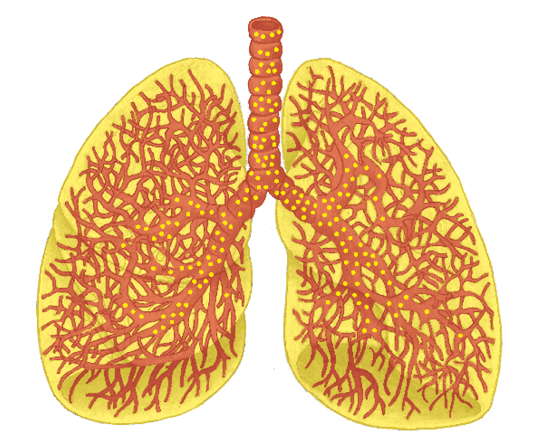
Goblet Cells (yellow)
Fear-of-suffocation conflict
Adeno-ca in situ of the lung, pulmonary tuberculosis
(PTB), pneumonia (Pneumocystis pneumonia, pneumocystis
carinii pneumonia, staphylococcal pneumonia, Klebsiella pneumonia, Legionnaire’s disease), pulmonary abscess1
We can survive for relatively long periods of time without food or drink. Without air, we are dead within three minutes. In nature, not getting air means the same as the end of life. This is why the alveoli trigger a fear-of-death SBS.
Deterioration of the alveolar tissue (pulmonary emphysema)
Same SBS as above. (See also: p. 197.) With an emphysema, the exchange of gases is reduced. This causes chronic respiratory distress (dyspnea) and shortage of oxygen (hypoxia).
| Phase | Recurring-conflict – The condition remains after many repair phases: if pulmonary nodules are degraded, holes in the tissue (caverns) normally remain (seen as circular shadows on an x-ray). Advancing emphysema causes more and more alveoli to lose their ability to function. |
|---|---|
| Therapy | Questions: see previous page. Find out what the conflict and conditioning are and, if possible, resolve them in real life so that the SBS comes to an end. Guiding principles: “I am safe.“ “The danger has passed.“ “I am safe in God‘s hands.“ Breathing exercises, stretching, gymnastics, yoga. MMS (see p. 68). Hydrogen peroxide (H2O2) 3% internally. Hildegard of Bingen: lungwort tea. Bring the herb to a boil and allow it to stand in the water. Drink it on an empty stomach for several days. Linseed oil. See also: the lung remedies on p. 208. |
Enlargement of the lungs, lymph nodes and connective tissue nodules
(pulmonary sarcoidosis, Besnier-Boeck disease)
Same SBS as above. (See also: p. 197.) Conflict possibly has a self-esteem-component: “I can‘t breathe well enough.“
In CM, this is seen as a so-called systemic illness of the mesoderm, with the lungs being the primarily affected organ.
From the viewpoint of the 5 Biological Laws of Nature, there are no such “systematic illnesses“ and thus, we look at the symptoms: enlargement of the lymph nodes on the lung stem points to a repair phase (CM: sarcoidosis stage 1). The conversion of functional lung tissue into connective tissue points to relapses (CM: sarcoidosis stage 3).
| Example |  The bike-riding student starts crossing a traffic light too early and is nearly run over by a car. Although nothing happens, he “sees his life flash before his eyes“ = fear-of-death conflict. The conflict recurs daily, since he crosses the same intersection everyday while riding to the university. After two years, he goes to the doctor because he has trouble breathing and coughs when he exerts himself. Diagnosis: sarcoidosis of the lungs. He is treated with 35 mg of cortisone per day but his lung volume remains at 70%. The conflict is resolved when he learns about the 5 Biological Laws of Nature and avoids the traffic light as his “therapy.“ The sarcoidosis retreats almost completely. The bike-riding student starts crossing a traffic light too early and is nearly run over by a car. Although nothing happens, he “sees his life flash before his eyes“ = fear-of-death conflict. The conflict recurs daily, since he crosses the same intersection everyday while riding to the university. After two years, he goes to the doctor because he has trouble breathing and coughs when he exerts himself. Diagnosis: sarcoidosis of the lungs. He is treated with 35 mg of cortisone per day but his lung volume remains at 70%. The conflict is resolved when he learns about the 5 Biological Laws of Nature and avoids the traffic light as his “therapy.“ The sarcoidosis retreats almost completely. (See www.germanische-heilkunde.at/index.php/erfahrungsberichte) |
|---|---|
| Phase | Recurring-conflict affecting the alveoli > formation of scar tissue. |
| Note | It is possible that the diagnosis of sarcoidosis is based on multiple bronchial scarring (this would be a recurring territorial-fear conflict). |
| Therapy | Questions: see previous page. Find out what the conflict and conditioning are and, if possible, resolve them in real life so that the recurring conflict comes to an end. Guiding principles: see above. See also lung remedy below. Breathing exercises, gymnastics, outdoor exercise. Hildegard of Bingen: millet mixed powder special recipe. In CM, for asthma, emphysema and sarcoidosis, the same drugs are given (bronchodilators, cortisone). In acute cases (repair phase crisis) they are practical and they are undoubtedly useful. Long-term intake is not recommended due to the side effects. |
1 See Dr. Hamer, Charts p. 21
Bronchial Musculature
Territorial-fear conflict
(motor)
Bronchial Mucosa
Territorial-fear conflict
Bronchial Goblet Cells
Suffocation-fear

Bronchial tumor (bronchial epithelial cancer)1
| Conflict | Territorial-fear or shock-fright conflicts (dependent on “handedness,” hormone levels and previous conflicts). A person is afraid of losing his territory (e.g., partner, job) or his position in the territory (position, level). “To have a terrible or mortal fear.“ “I was scared to death.“ “I am terrified!“ The territorial-fear conflict is an active/male reaction to a threat to his territory. The shock-fright conflict is a passive/female reaction to the same thing (typically, the male reacts with attack, the female with passive fright). |
|---|---|
| Examples | A woman has a husband, who is always being unfaithful. She is never sure whether or not he is having another affair = territorial-fear conflict with degradation of cells from the bronchi in the active phase. She comes into healing when she separates from him and meets another man who loves her passionately and deeply. With this new partner, she is sure that he is true to her. Restoration of the bronchial mucosa = bronchitis or a bronchial ca. (Example from Ursula Homm) A family father has a job in a small plumbing company and is two years away from his retirement. He has a good, friendly relationship with his boss. One day, the boss decides to join up with a new business partner. The new partner cannot stand the patient. The relationship worsens and the patient is afraid of being fired. This would be very bad, as he still has two young daughters to raise and moreover, he wouldn‘t be able to get a new job at his age = territorial-fear conflict. Before he goes into retirement, in other words, two years later, his fear of losing his job dissolves. He begins to cough and thinks he has bronchitis. When his symptoms do not improve he gets a lung x-ray. The diagnosis: “cancer of the bronchi.“ This causes him to have a fear-of-death conflict. Finally, the patient dies after receiving all possible therapies. (See Claudio Trupiano, Danke Doktor Hamer, p. 327.) ➜ Also, often a threat to one‘s “time territory.“ For example, someone is put under time or schedule pressure. Someone‘s time is “robbed“ from them or someone else decides what will be done with their time. A 26-year-old, left-handed man starts up a small company with a friend. After a while, they begin to have major arguments about how their presence at the firm should be regulated. The patient wants to take advantage of his entrepreneurial freedom with flexible, need-oriented working hours. His partner insists on an exact work schedule = territorial-fear conflict regarding the larynx (left-hander). After an unpleasant separation from his business partner, the patient can choose his own hours, and the conflict seems resolved. Unfortunately, a trigger remains: whenever he is pressured with private or business appointments, he subconsciously remembers the old stress and reacts with territorial-fear. The day after the appointment, he has a congested larynx and a hoarse voice = repair phase of the larynx mucosa. (Archive B. Eybl). For the last 30 years, a 47-year-old mother of two has met with her “best friend“ twice a week. In the last half year, however, her friend has suddenly stopped seeing her. After several futile attempts to contact her, she gives up, disappointed = territorial-fear conflict – “My friend is leaving my territory.“ She comes into healing when her friend phones her to wish her a happy birthday and she confronts her on the matter. Now, she can close the books on the subject. A week later, she contracts pneumonia. (Archive B. Eybl) For another example see “22 brain metastases” p. 41. |
| Conflict-active | Functional limitation; later, cell degradation (ulcers) of the bronchial mucous membrane, usually unnoticed. Simultaneous slackening of the, according to Dr. Hamer, striated musculature. The affected area can be anywhere from the beginning of the trachea into the smallest branches of the bronchi = CM‘s “ulcerating bronchial cancer.“ |
| Bio. function | Expanded bronchi due to lax ring musculature. This allows the person to improve their intake of air, so they can defend the territory more effectively. One can “scream” everyone else out of their territory – shout louder during a dispute. |
| Repair phase | Restoration of the bronchial and/or tracheal mucosa = inflammation of the bronchi (bronchitis), pneumonia, bronchial cancer: swelling, reddening, cough, possibly bloody sputum, and pain; strong swelling with exhaling difficulties during syndrome. Due to the swelling, an entire section of the lung can be cut off temporarily from the breathing process (= insufficient-ventilation atelectasis). As soon as the swelling is reduced, the air passage opens up again, that is, the atelectasis disappears again. Longer lasting bronchitis is due to a recurring–conflict. |
| Repair crisis | Cough and/or coughing cramps due to participation of the bronchial musculature, chills. |
| Note | Bronchial cancer is usually diagnosed in the repair phase, often together with syndrome. |
| Questions | When did the symptoms begin? Which territory is this about? (Partner, residence, workplace)? What stressed me at the time in question? What am I thinking about when I can’t sleep? Dreams? (Indication of the conflict). What keeps me from dealing with the issue better? Was one of my ancestors confronted with a similar situation? What is continuing on, down through the generations? Which conditioning sensitizes me? What beliefs lead me to the dilemma? Am I ready to start over? |
| Therapy | If still conflict-active: Determine and resolve the conflict, conditioning and beliefs. Enzyme preparation, lymphatic drainage. Hildegard of Bingen: ground ivy elixir special recipe. Vitamin D3, cod liver oil (see p. 68), hydrogen peroxide (H2O2) 3% strength internally. See also lung remedies p. 208 If necessary: OP, if the tumor is too large and/or large bronchial branches are affected. |
Inflammation of the bronchi (bronchitis)
Same SBS as above.
| Phase | Repair phase: Restoration of the squamous mucous membrane. Pain, narrowing of the bronchi (stenosis) or closure (atelectasis) due the healing-swelling, breathing noises (stridor). Expectoration of phlegm (sputum). Cough = repair phase crisis of the bronchial musculature. The cough‘s biological purpose is to expectorate the mucus. |
|---|---|
| Note | By recurring–conflict or in persistent repair, CM speak of “chronic hypertrophic bronchitis.“ A “bronchial cancer“ might just as well be diagnosed, should a lung x-ray be taken. |
| Therapy | The conflict is resolved. Support the healing and avoid relapses. Saltwater or tea inhalations. Tea: horehound, marshmallow, Iceland moss, mallow, primrose, mullein, elderberry. Colloidal silver internally. In the repair phase crisis, black tea or coffee. Possibly CM – cortisone, anticonvulsants. See also: lung remedies p. 208. |
Bulging or widening of the bronchi (bronchiectasis)
Same SBS as above. (See: p.200). According to CM, chronically recurring inflammations can degrade the structure of the bronchial wall.
Symptom: expectoration of large amounts of phlegm upon arising in the morning.
| Phase | Recurring, persistent-active conflict with local cell degradation from the bronchial mucosa > a thinning and subsequent bulging out of the membrane. During the periods between the repair phases, there is increased phlegm with coughing in the repair phase crisis. |
|---|---|
| Therapy | Questions: see above. Find conflict and conditioning and resolve them in real life, in order to prevent relapses. See also: lung remedies on p. 208. |
Inflammation of the trachea (tracheitis), tracheal cancer (tracheal-epithelial cancer)
Same SBS as above. (See: p.200). With regard to conflicts, the mucosa of the trachea belongs to the bronchi.
| Phase | Repair phase: Restoration of the squamous mucous membrane. Pain under the breastbone. Possibly narrowing of the trachea (tracheal stenosis) due to repair-swelling especially with syndrome. If the cell degradation was long and intense, the healing can also take a long time. This is possibly the manifestation of a recurring conflict. In both cases, tracheal cancer may be diagnosed. |
|---|---|
| Therapy | The conflict is resolved. Support the healing. Avoid recurrences. In the repair phase crisis, possibly CM: cortisone, anticonvulsants. If necessary: surgery. See: lung remedies on p. 208. |
1 See Dr. Hamer, Charts p. 111
Chronic obstructive pulmonary disease (COPD)
COPD is a collective term for various chronic diseases of the lungs. This mainly includes emphysema and chronic bronchitis.
The diagnosis is mainly based on testing lung function (spirometry).
The diagnosis is, in our view, relatively meaningless, except for the term “chronic“ > recurring SBS of the alveoli and/or recurrent SBS bronchi.
For therapy, see the respective SBS on p. 197 or p. 200.) If applicable, cannabis oil.
A 62-year-old worker, a passionate hiker, notices that he is getting less and less air while walking. According to his spirometry, his lungs are functioning at 54% – suspicion of COPD.
During his first consultation with a New Medicine therapist, it becomes clear that he simply has laryngeal asthma (clearing his throat often and whistling sounds at night).
Cause: He can’t tolerate orders. Unfortunately, he’s always getting them from his boss at work and from his partner.
Therapy instructions from his only appointment: “Don’t accept any more commands. Look forward to your pending retirement. Enjoy and internalize any feelings of freedom at every opportunity.” Two years later: With the exception of one short relapse six months later, the patient has remained symptom-free. (Archive B. Eybl)
Narrowing of the bronchi (bronchial asthma), spastic
bronchial inflammation (spastic bronchitis)1
Bronchial asthma causes difficulties in exhaling > slow and heavy exhalation. If the mucosa and muscles are affected, the condition is accompanied by bronchitis and bronchial stenosis.
| Conflict | Territorial-fear conflict or shock-fright and speechlessness conflict in the repair phase crisis. Additionally, an active conflict or a repair phase crisis on the opposite, left, cerebral cortex side. (For conflict explanation, see: p.200). |
|---|---|
| Examples | When he was a child, a 33-year-old, right-handed, asthmatic patient had to listen to the intense arguing of his parents. The parents then separated = territorial-fear conflict affecting the bronchi, shock-fright conflict affecting the larynx, and stinking conflict affecting the mucous membranes of the nose. All three conflicts led to cell degradation in the active–phase and restoration in the repair phase. The patient has several triggers: dampness or warm-damp weather, arguments, separations, and disharmony of all sorts. Due to the triggers, he repeatedly comes into conflict activity and then into repair with the symptoms of asthma and sniffles. (Archive B. Eybl) A 60-year-old, right-handed retiree with two grown children has had a cat allergy, since his 18th birthday. Whenever he is near a cat for longer than half an hour, the bronchi tighten up and he cannot breathe properly – although he loves cats! Moved to tears, he recalls the original conflict 40 years ago: His favorite cat often stole food from the table. Once, his mother caught the cat “in the act“ and hit it so hard that the cat slunk into the cellar. After that, the cat had nothing to do with any family member other than him = territorial-fear conflict. Subsequently, he always went down into the cellar and pet his cat. It then licked his temples with gratitude. Later, the cat died. Additional finding: The patient has a basal-cell carcinoma (skin cancer) on the temple, just on that spot = for the last 40 years, a hanging-separation conflict – the skin contact with the cat was broken off. Note: The patient‘s cat allergy is based, like all allergies, on a trigger. For this man’s subconscious, cats are an alarm signal: Watch out! Something bad could happen again > start-up of a bronchial SBS > relaxation of the bronchial musculature in the active–phase > cramping up in the repair phase crisis = CM: “asthma.“ (Archive B. Eybl) |
| Conflict-active | Degradation of the bronchial musculature (muscle necrosis) > muscle weakness. Simultaneously, cerebral cortex-controlled reduction of innervation > motor paralysis. In the case of a coupled conflict, simultaneous degradation of bronchial mucosa – all largely symptomless. |
| Bio. function | Widening of the lumen in the bronchi due to “relaxed“ bronchial musculature > get air better and faster. |
| Repair phase | Restoration of bronchial musculature and return of innervation, tickling irritation in the throat. With coupling, simultaneous bronchitis with expectoration. |
| Repair crisis | Bronchial asthma attack: coughing fits, longer exhalation and/or exhalation together with coughing, lasting from several minutes to a maximum of three days. Narrowing (tightening) of the bronchi and/or trachea, possibly with wheezing sounds (stridor trachealis) when breathing. |
| Note | An attack occurs when a conflict is active on the opposite, left half of the cerebral cortex or also in the repair phase crisis. Only this constellation makes bronchial asthma possible. By allergic bronchial asthma, the conflict is started up briefly due to a trigger (= CM’s allergen). |
| Therapy | Questions: see: p.201. Determine the conflict and conditioning and, if possible, resolve them in real life. Guiding principles: “I am safe.“ “I am in the hands of God.“ Breathing exercises, dancing, singing. MMS (see p. 68). Hydrogen peroxide (H2O2) internally. Vitamin D3, cod liver oil (see p. 68). In the repair phase crisis black tea or coffee, possibly: CM cortisone, antispasmodic and bronchodilators. Long-term use is not recommended because of side effects. |
1 See Dr. Hamer, Charts pp. 111, 112
Goblet cell tumor (adeno-ca), excess phlegm (mucus) in the bronchi1
From a developmental standpoint, goblet cells are descendants of the intestinal mucosa glands. They are responsible for the lubrication and moistening of the air passages.
| Conflict | Chunk conflict (explanations see: p.15, 16). not being able inhale, moisten the air. In practical terms: suffocation fear, blocked airways (foreign objects, artificial respiration). “I’m not getting any air.“ “I’m struggling for air.“ |
|---|---|
| Examples | For the last year, a 28-year-old mother is so congested that it causes her to vomit regularly. Her only son was born prematurely and suffers from respiratory problems among others. One night, he nearly suffocated in her arms – she called an ambulance much too late. Since then, she always listens in the night to hear if her little one is breathing normally. Substitute suffocation conflict for her son affecting the goblet cells. When the connection was explained to her, she was able to completely accept her son’s difficulties and, for the first time, appreciate herself as the good mother that she is. Relieved, she subsequently spent several nights soaking the sheets with sweat and coughing up yellow sputum. Afterwards, her symptoms were gone. (Archive B. Eybl) ➜ The umbilical cord of an infant is cut too soon > insufficient oxygen supply to the baby. ➜ While having an asthma attack, a person thinks he is suffocating. ➜ A person is exposed to an extreme amount of dust or smoke (fire dept., mining, stone cutting, etc.). |
| Conflict-active | Increased function, cell proliferation of the goblet cells (goblet cell tumor) = in CM: chronic cartarrhous bronchitis, intrabronchial goblet cell adeno-ca, goblet cell hyperplasia = excess phlegm due to increased production of mucus. |
| Bio. function | Better breathing and/or dust expulsion due to more bronchial mucus. |
| Repair phase | Normalization of function. If fungi or bacteria (mycobacteria) are present > tubercular-caseating degradation or small goblet cell “tumorlets.“ Expectoration of yellow (purulent) mucus, mild fever, night sweats, halitosis. |
| Note | This SBS is rare. It is difficult to draw the line between this disease and bronchitis (territorial-fear conflict), which is also accompanied by excess mucus. Decisive sign: proof of bacteria (laboratory), expectoration of yellow, purulent sputum, night sweats accompanying goblet cell carcinoma degradation. This SBS would explain why asthmatics, who are regularly afraid of suffocating, often suffer from extreme congestion. |
| Questions | Congestion since when? (Conflict previous). Suffocation fear from what? (Own asthma or that of a loved one, dusty workplace, artificial respiration, etc.)? What has sensitized me? What did my parents/ancestors experience? (Miners, lung disease)? Did the pregnancy or birth play a role? |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life. Tea: horehound, anise, fenugreek, speedwell, linseed, ground ivy. MMS (see p. 68). Vitamin D3, cod liver oil (see p. 68), black cumin. Colloidal silver internally. Hildegard of Bingen: special recipe: blackberry elixir. See also: lung remedies p. 208. |
Cystic fibrosis (CF = mucoviscidosis, drying up of the bronchial mucus)1
| Phase | Persistent repair, usually recurring in infancy > more and more goblet cell functional tissue is “melted away“ – converted to connective tissue. This causes less mucus to be produced or its production stops altogether = mucoviscidosis. |
|---|---|
| Therapy | Find out what the conflict and conditioning are and, if possible, resolve them in real life so that the persistent repair can come to an end and the goblet cells can regenerate. Lymph drainages (p. 68), acupuncture, acupoint (see p. 68) and classic massage, colloidal silver internally. See also: lung remedies p. 208. |
1 See Dr. Hamer, Charts p. 21
Coronary Veins (blue)
Female-sexual loss-
of-territory conflict
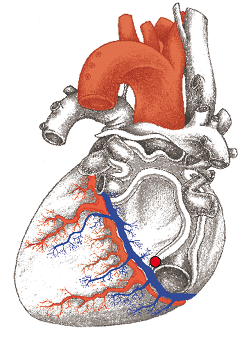
Occlusion of the lung artery (pulmonary embolism, thromboembolism)1
This “disorder” should actually belong to the chapter on the heart, because the lung only receives the effects of a heart SBS. According to CM, the blood clot (thrombus) that leads to a lung embolism is transported from the leg veins.
However, Dr. Hamer found out that in a pulmonary embolism, the thrombus originates in a venous shank of the coronary vessels (coronary veins). According to my experience, this explanation does not account for all lung embolisms. In all likelihood, some of the blood clots do break away from the deep leg veins (SBS of the Veins s. p. 176). For individual cases, a diagnosis based on the symptoms shouldn’t pose a problem. The following describes a clot departing from a coronary vein:
The blood supply of the heart: Via the coronary arteries, the heart muscle is supplied with oxygen-rich blood. After the gas exchange in the heart’s muscle tissue, the coronary veins take the oxygen-poor blood into the right atrium. From there, it goes into the right ventricle and then via the pulmonary artery (albeit with oxygen-poor blood) into the lungs for new oxygen enrichment. Now the decisive point: If any clot is released from the coronary veins, it will becomes lodged in a pulmonary artery = lung embolism.
1 See Dr. Hamer, Charts p. 126
Right
cancer

Left
cancer


Branchial Arches
Frontal–fear conflict
Small cell bronchial (lung) cancer
In CM, this kind of tumor is seen as a bronchial tumor. However, as Dr. Hamer found out, we are dealing with an SBS of the branchial arches or with callus (bone fluid) leaking from an injured bone in the area. Vertebrae, ribs or the sternum come into question. (See osteosarcoma p. 358). Due to its inaccessible location in the middle of the chest cavity, this tumor is considered inoperable by CM and hardly curable.
| Conflict | Frontal-fear conflict. Fear of approaching, inescapable danger coming towards us and we cannot evade it (also see p. 181.) Or powerlessness conflict. One cannot stop something bad from happening. Time is running out. One doesn’t do anything (but must) and is tense for this very reason (see p. 147). |
|---|---|
| Examples | A 43-year-old, right-handed, happily married patient has a 12-year-old son. One day, the father has to have a meniscus surgery. When he wakes up from the anesthesia, his wife informs him that his son is hospitalized, having badly injured his head diving head first into water. The next day, he learns that his son will have to undergo surgery. His life is in danger > still in the hospital, the patient suffers a frontal-fear conflict because of the oncoming danger (the surgery) and a fear-of-death conflict – both conflicts in substitution for his son. He feels the urge to jump out of the window if the boy should die (high conflict-intensity). In the repair phase, he feels a downwards pull in the left ear toward the neck and breastbone with strong pressure and squeezing. Just above the collar bone, a cyst has developed (= branchial arches in healing). He also sweats heavily during the night and coughs blood (= alveoli in healing). The hospital’s explanation of the symptoms is a diagnosis of an alveolar cancer and a small-cell bronchial cancer. (Archive B. Eybl) |
| Repair phase | Cell division, restoration of the branchial arches = CM: small-cell bronchial cancer. This progression is described on p. 181 under non-Hodgkins lymphoma. |
| Questions | Did I feel an indication of this under my breastbone, possibly long before the diagnosis was made? (= Beginning of the conflict). Which danger is this about? Is the issue permanently resolved? (Exclude the possibility of recurrence). |
| Therapy | The conflict is resolved. Support the healing. Guiding principles: “The danger is over. I am safe.“ Lymph drainages (see p. 68). It is crucial to overcome the shock of the diagnosis and leave the fear behind. |
Water in the lungs (interstitial or alveolar pulmonary edema)
It is typical for patients with water in the lungs to only sleep in a sitting position – at least in this position they have the upper part of the lungs to breathe. We can hear the typical rattling noise as the patient breathes. This serious symptom is a sign of poor general health. Principally, the kidney collecting tubules are always involved with this. The following causes come into consideration:
- Pulmonary edema due to poisoning: Irritant gases (chlorine, ammonia, hydrochloric acid, etc. = acute pulmonary edema), drugs (heroin, methadone), chemo-poisoning > destruction of the alveoli and capillaries > leakage of fluid into the lungs = pulmonary edema.
- Weakness of the left ventricle (heart failure): Overwhelmed conflict > backflow of blood into the pulmonary circulation> leakage of blood plasma in the pulmonary capillaries > water in the lungs = most common cause of lung edema (see: p.154).
- Repair phase bronchial mucosa: Territorial-fear in repair: Inflammation of bronchial mucosa = bronchitis > pulmonary edema during syndrome (see: p.200).
- Repair phase alveoli: Fear-of-death conflict: Inflammation of the alveoli lung tuberculosis > exudation of pus and water > pulmonary edema during syndrome (see: p.197).
Therapy
In accordance with the cause. Both acute and chronic pulmonary edema need treatment. Definitely consider: therapeutic measures for kidney collecting tubules p. 277. See also: lung remedies p. 208.
Whooping cough (pertussis)
According to CM, whooping cough is caused by the bacterium Bordetella pertussis, and is one of the so-called pediatric diseases. Whooping cough comes from either the larynx or the bronchial muscles.
- Cause larynx: repair phase crisis of the laryngeal musculature or irritation (= tickle, urge to cough) of the laryngeal mucosa in the repair phase = shock-fright conflict. (See: p.195.)
- Cause bronchi: repair phase crisis of the bronchial musculature or irritation of the bronchial mucous membranes in the repair phase = territorial-fear conflict. (See: p.203.)
In both cases, the coughing has a biological function of expectorating the phlegm generated by the inflammation. Whooping cough attacks are especially serious in combination with syndrome.
Therapy
The conflict is resolved. Support the repair phase.
By attack (repair phase crisis): stand up, go where it is cool, drink cold beverages, tea, coffee, possibly CM: cortisone, antispasmodic, bronchodilators.
Tea: hibiscus, ivy, thyme, English plantain, peppermint.
By recurring-conflict: breathing exercises, sunbaths, solarium, sauna, infrared cabin, damp chest compress.
Black lung disease (pneumoconiosis; silicosis, asbestosis)
This is one of the most commonly occurring occupational illnesses.
To a certain extent, dust is intercepted by the mucous membranes of the nose, throat, windpipe, and bronchi. With the help of the cilia (tiny hairs), these particles are transported outward or coughed up. The smallest or thin, fibrous particles, however, can make their way as far as the bronchioles and remain there. The very smallest particles can even enter the alveoli. There, the body builds connective tissue around them, which, in and of itself, is not harmful. If, however, over the years and decades, dust is continually inhaled, this scar tissue takes up more and more space so that the performance of the lung is eventually diminished. One speaks of a fine-particle-induced “pulmonary fibrosis“ > not a conflict but damage caused by dust. The growths of connective tissue are often interpreted as “cancer.“
Dust inhalation can also be perceived as an attack conflict as can the diagnosis “black lung.“ (See: p.209.)
Therapy
Stop breathing in dust. Guiding principle: “My lungs are full of light and energy.“ Breathing exercises, gymnastics, sport for cleaning the lungs. See also: lung remedies.
Smoking and the lungs
It is clear that smoking is not healthy. It pollutes the breathing passages with tar and soot. Nicotine and other ingredients are taken up by the body and they poison it gradually from within. Nicotine, like all drugs, makes us temporarily sympathicotonic = “high.“
For the “good feeling“ that comes from smoking, we pay a high price: the loss of freedom (due to addiction), loss of vital energy due to a bad conscience and local and general contamination.
However, the commonly accepted maxim, “Smoking leads to lung cancer,“ is wrong. The signal for cell division in the bronchi and alveoli comes from the brain. There is no cell division without the brain ordering it to happen. Why is it that lung cancer is diagnosed more often in smokers?
- Smokers‘ lungs are examined more often because of contamination – symptomatic coughing or as a “precaution.”
- Doctors intentionally examine smokers more often for lung cancer. Swollen, inflamed, sooty, scarred bronchial epithelium is designated as “cancer.“
- Many smokers believe that they will get cancer because they smoke. Mandatory warnings reinforce this belief. Whoever continues smoking with this on their mind will eventually suffer a fear-of-death conflict and be responsible for their own undoing.
Therapy
Quit smoking. If possible, quit without being forced to do so. Brutal withdrawal harbors considerable conflict potential.
Guiding principle: “I am free and independent! This is real quality of life.“
Lung remedies
- Regular breathing exercises.
- Aerobic exercise.
- Tea: horehound, lungwort, fir needle, agrimony, sage, plantain, knotgrass.
- Pelargonium root extract (Kaloba®).
- Cayce: horehound syrup.
- MMS (see p. 68).
- Hildegard of Bingen: goat‘s milk.
- Hydrogen peroxide (H2O2) 3% internally.
- Sunbathing.
- Vitamin D3, cod liver oil (see p. 68).
- Cannabis oil (CBD oil).
All experience reports on the organ system « Lungs, bronchi and trachea » from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2026/03/25   A brief healing phase of a territorial anxiety conflict (cough) and a more intense healing of a chunk conflict in a 3-year-old (vomiting) | Territorial anxiety conflict, chunk conflict | ||||
 | 2026/02/25 I had always liked cats, but growing up in an apartment building where larger pets were prohibited, there were no cats in the neighborhood. At almost 50, I suddenly realized that I was allergic to cats, as more and more relatives, acquaintances, and even neighbors suddenly had cats... | |||||
| 2026/02/25 I had hay hayfever since I was 14 years old. At times, I also had asthma. When I was 19, I had just met someone new who invited me to spend a weekend at his relatives' farm. I was looking forward to it and went with him... | |||||
 | 2025/11/10 A few hours after learning of the sudden death of his neighbor, he began experiencing fever, extreme sweating, and severe discomfort for an entire month... | |||||
| 2025/11/10 During his summer vacation on the Baltic Sea, he had a terrible experience in which he and his son almost drowned. They were having fun jumping into the high waves when they got caught in a rip current that pulled them out to sea. | |||||
 | 2025/09/07  Case of allergy resolved after a separation conflict, treated with ocular reprogramming, resulting in disappearance of symptoms. | Separation conflict, skin, respiratory mucosa, allergy, ocular reprogramming | ||||
 | 2025/08/16 The reason Sergej (name changed) consulted me for help was because of his panic attacks while driving. During the anamnesis, he reported that he could no longer drive a car or truck for more than about 15 minutes... | |||||
 | 2025/08/01 The following symptoms started 11 days ago: runny nose, laryngitis, mucous build-up in the right lung with green-yellow sputum. I feel exhausted and have slight aching limbs. This long course of illness is completely uncharacteristic for me ... | pulmonary tuberculosis | ||||
2025/02/22 Rhea has coughed constantly for most of her life - no medication or therapy has worked in the long term. In an exchange with 5BN/GNM practitioner Danny Carroll, she did intensive research into her life and found out that there were phases in her life from time to time when she didn't cough. And it was always when she was not in a committed relationship ...  | ||||||
 | 2024/12/13 For 22 hours my mother's biology was in a frenzy! This was followed by a severe bout of bronchitis. | fear of territory / fear of fright, bronchial tubes | ||||
2024/11/05 In this experience report video, our course participant talks about his successful resolution of a horse hair allergy based on the 5 Biological Laws of Nature. For 35 years he had severe symptoms on contact with horse hair and was able to find and resolve the causal situation! Congratulations and thank you very much for sharing this valuable experience!  | ||||||
 | 2023/08/26  This case describes the healing of an already advanced thyroid tumor with the conventional medical diagnosis: death.... and the resulting lung cancer. Which we have also got under control. | |||||
 | 2023/08/20  This is a case that occurred in a family with three children: 6 years, 4 years and 6 months. The eldest constantly takes the infant in her arms, although the mother does not welcome it. But the six-year-old sister breaks the ban from time to time. | chunk conflict, anger, trouble; territorial threat | ||||
| 2023/04/10 When the PLANdemie was announced on Swiss television in March 2020, I knew immediately that it was a lie and a scam. My key sentence was: “They want to sell us the vaccine.” That was the start of the agitation and mistrust against me ... | |||||
2022/07/31 Sima talks about her successful resolutions of her birch pollen and cat hair allergies based on the 5 Biological Laws of Nature in this testimonial video. Congratulations and thank you very much for this nice report!  | Track, resolving allergies | |||||
2022/05/25 These are the testimonials (in short) about the next six successfully resolved allergies of the participants of our practice course "Resolving Allergies". The reports are available as text and video.  | Track, resolving allergies | |||||
2021/09/07 These are the testimonials (in brief) about the next six successfully resolved allergies of the participants of our practice course "Resolving Allergies". The reports are available as text and video (the video is in german, but has english subtitles).  | Track, resolving allergies | |||||
2021/08/20 These are the testimonials (in brief) about the next six successfully resolved allergies of the participants of our practice course "Resolving Allergies". The reports are available as text and video (the video is in german, but has english subtitles).  | Track, resolving allergies | |||||
 | 2021/08/01 Case of an Italian Franciscan monk who rebuilt an old, dilapidated monastery in the vast surroundings of Assisi and experienced bronchitis with allergic alveolitis, after this project, which was a lifelong dream of him, was first threatened by his order who agreed later. | |||||
| 2021/07/25 A mother comes for treatment and tells me that she is very worried about her 4-year-old son because he is highly allergic to nuts. He has already had to go into intensive care twice due to shortness of breath or swelling of the airways ... | Allergy | ||||
2021/06/30 These are the testimonials (in brief) of the first seven successfully resolved allergies of the participants of our practice course "Resolving Allergies". The reports are available as text and video (the video is in german, but has english and spanish subtitles):  | Track, resolving allergies | |||||
| 2021/06/30 The case showed well how programs got going as follow-up activations: Jonny had a cough with blood sputum. He was to be examined for "lung carcinoma" by means of biopsy. In the biopsy, the needle is inserted through the back. Without anesthesia, because he was told that this "goes so fast, you don't need anesthesia". | Lung carcinoma, mesothelioma, pulmonary nodule, Consequential conflicts, | ||||
2021/06/17 For 20 years, there have been several situations in his life when he has reacted with epilepsy-like symptoms: First, when he has been frightened. Second, when he has felt strong emotions such as fear, sadness, fatigue or even euphoria. And, interestingly, also and especially strongly when the hamstring reflex test was performed during examinations. Once the causative event was found 20 years ago, the symptoms could be successfully resolved afterwards. | ||||||
2021/05/07 Massive symptoms in the context of the corona crisis with cause in the compulsory masking measures and orthodox medical "Covid-19" diagnosis. | ||||||
| 2020/06/14 Two weeks ago I met my cousin and she told me that one of her twin sons had been coughing a lot for a few days and was having difficulty breathing. She went to the doctor, who diagnosed the 5-year-old with pneumonia involving the larynx ... | Territorial anxiety conflict | ||||
| 2020/03/22 In the 3rd/4th week of pregnancy, the couple go on vacation to a hotel in Egypt, where the mother experiences two fear-of-death conflicts - and the baby along with her. The baby is to be operated on by two teams of doctors immediately after birth. It may be necessary to remove an entire lung, as one is completely infested with cysts. The parents manage to resolve and reduce the symptoms in good time before the birth. | Fear of death conflict | ||||
| 2019/07/08 Harassment and threats by instructors in the People's Army, since then recurrences in various situations. | Cough, dry, chronic | ||||
2017/12/18   Resolution of my dust mite allergy with allergic asthma, which has been with me more or less intensive since babyhood for almost 30 years. 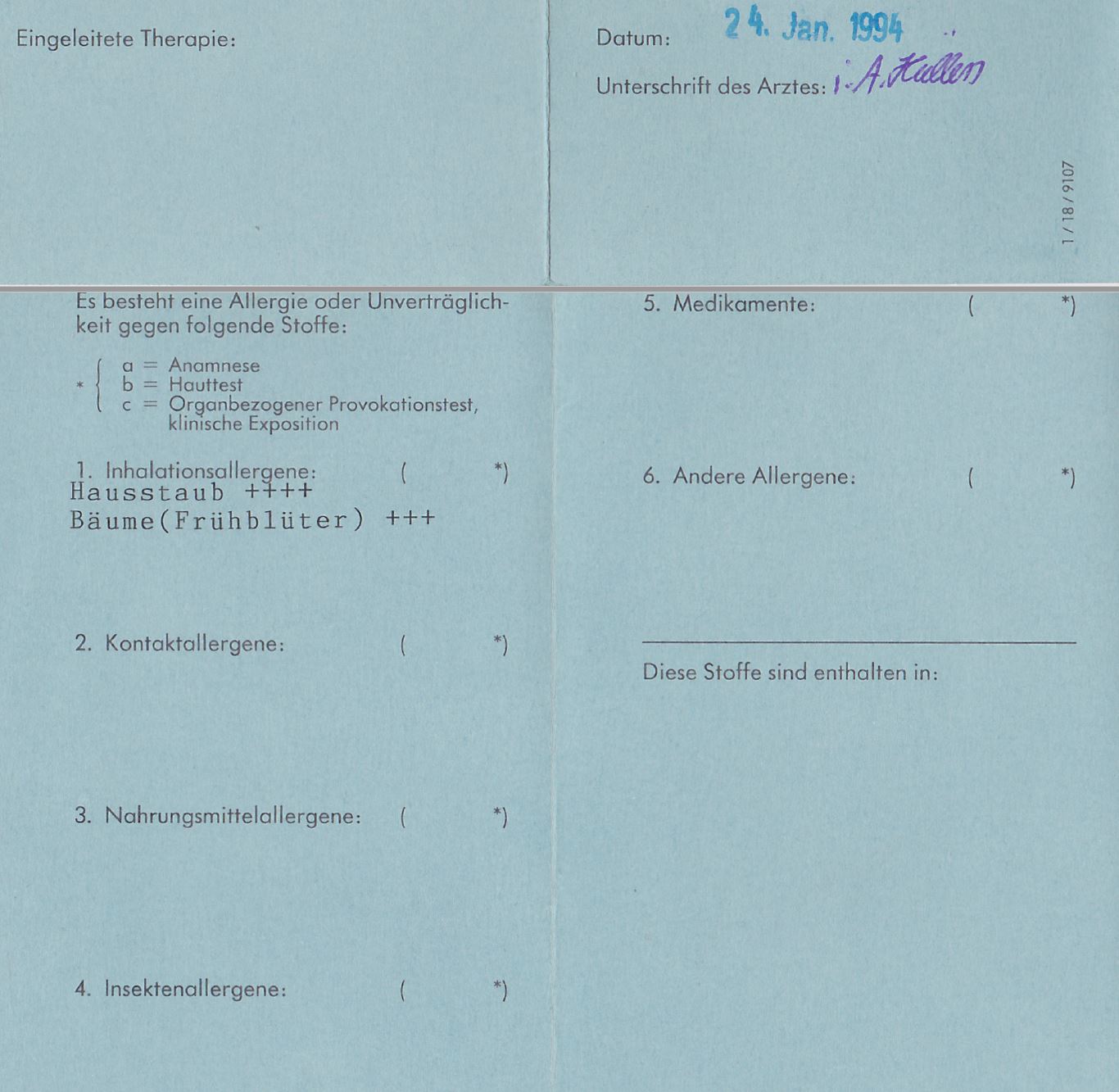 | Track, asthma, resolving allergies | |||||
2015/01/29 The client reacted with the bronchial mucosa as a result of a "fright" accident experience and experienced severe "bronchitis" after conflict resolution. By knowing the exact cause, the duration of the symptoms could be accurately determined and predicted. | ||||||
| 2015/01/01 Here is a list of other sources where experience reports with the 5BN can be found, e.g. to:: Bursitis, conjunctivitis, rheumatism, diabetes, hay fever, psoriasis, bedwetting, stuttering, oceans, aggressive constellation, endometrial CA, cervical cancer, shingles, tinnitus, toothache, heart attack, high blood pressure, colic, slipped disc, knee pain, leukemia, bone cancer, voice gone, stomach pain, hives, Epilepsy, intolerances, Crohn's disease, skin rash, facial paralysis, hiccups, anorexia, bronchitis, corneal inflammation, migraine, thyroid cyst, aphthae, osteolysis, gastritis, rectal spasms, milk duct carcinoma, allergies, hepatic coma, gray hair, nail fungus, heartburn, nasal polyps, caries, heart attack, ankylosing spondylitis, melanoma, psoriasis, water belly, hailstones, prostate, . .. |